29 Jan |
11:53 AM

For years, parents were told to wait until their child was two or three before giving them peanut butter. It seemed like the safest move-after all, peanut allergies can be deadly. But that advice, once backed by the American Academy of Pediatrics, actually made things worse. Between 1997 and 2010, peanut allergies in U.S. kids more than quadrupled. What no one realized then was that keeping peanuts away wasn’t protecting kids-it was setting them up to react.
The Turning Point: What the LEAP Study Changed
Everything shifted in 2015 with the release of the Learning Early About Peanut Allergy (LEAP) study. Led by Dr. Gideon Lack at King’s College London, this landmark trial followed over 600 high-risk infants-those with severe eczema or egg allergy-from infancy to age five. Half were given peanut-containing foods regularly starting at 4 to 6 months. The other half avoided peanuts entirely. The results were shocking: by age five, only 1.9% of the group that ate peanuts developed an allergy. In the group that avoided them? 13.7%. That’s a 86% drop in allergy risk. It wasn’t a small effect. It was a revolution. The National Institute of Allergy and Infectious Diseases (NIAID) quickly updated its guidelines in 2017, and since then, 26 major medical groups-including the AAP-have adopted the same approach. The message is clear now: early exposure isn’t risky. It’s preventive.How to Introduce Peanuts Based on Risk Level
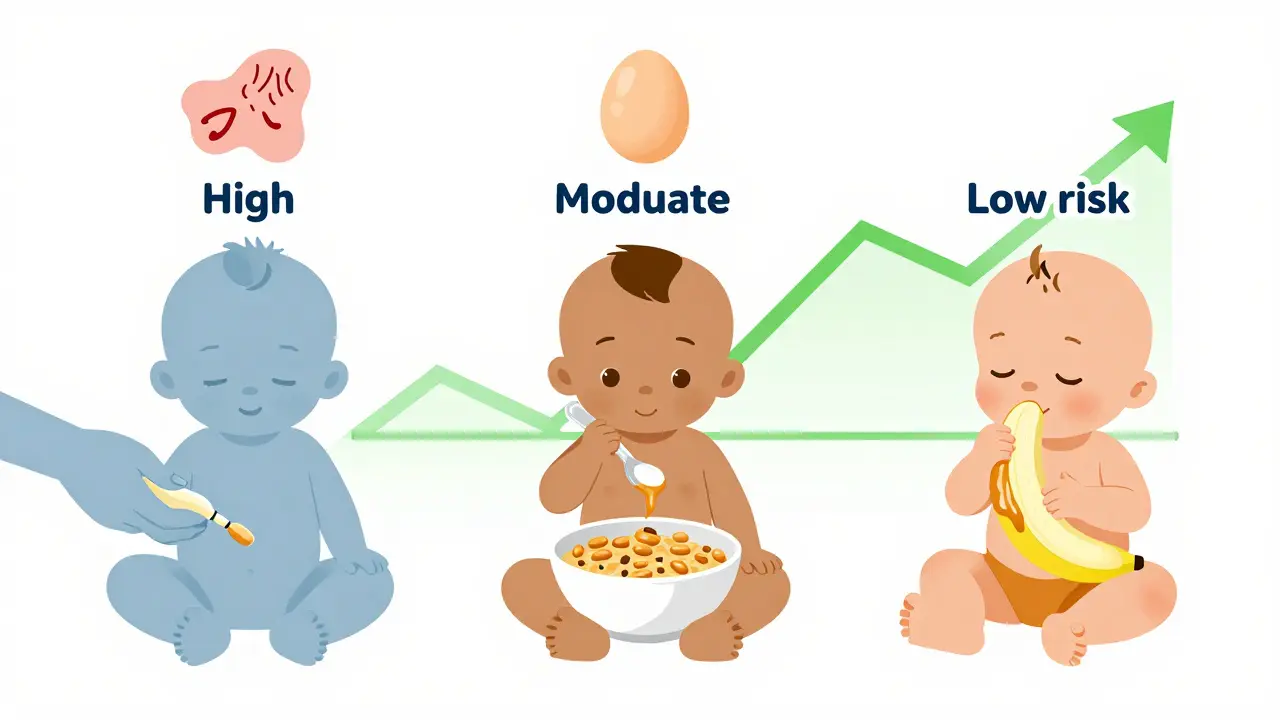
Not all babies need the same approach. The current guidelines divide infants into three risk groups:- High-risk: Babies with severe eczema, egg allergy, or both. These kids should be evaluated by a doctor or allergist between 4 and 6 months. If allergy tests come back negative, they start eating 2 grams of peanut protein-about 2 teaspoons of smooth peanut butter-three times a week. The first dose is often given in a clinic for safety.
- Moderate-risk: Babies with mild to moderate eczema. No testing is needed. Just start introducing peanut-containing foods around 6 months, at home, following the same 2-gram, three-times-a-week rule.
- Low-risk: Babies with no eczema or food allergies. Introduce peanut whenever you start solids-usually around 6 months. No special steps needed.
What Forms of Peanut Are Safe?
This is where parents get confused. Whole peanuts? Never. They’re a choking hazard. Peanut butter with chunks? Too risky for babies under one. The safest options are:- Smooth peanut butter thinned with water, breast milk, or formula
- Peanut powder mixed into pureed fruits, vegetables, or infant cereal
- Spoonable peanut butter pouches (designed for babies, low-sugar, no added salt)
- Bamba (a puffed corn snack with peanut, popular in Israel and now available in the U.S.)
Why Early Introduction Works-And Why Delaying Doesn’t
The science behind this isn’t just about exposure. It’s about training the immune system early, before it learns to see peanut as a threat. When a baby’s gut and skin barrier are still developing, introducing peanut protein helps the body recognize it as food-not a danger. Studies since LEAP have confirmed this. A 2023 meta-analysis of LEAP and the EAT study found that babies who ate peanut before six months had up to a 98% lower chance of developing an allergy-if they stuck to the plan. Even in the real world, where not everyone follows perfectly, the risk dropped by 75%. Compare that to the old way: waiting until age two or three. That strategy didn’t just fail-it made allergies more common. The U.S. saw a steady climb in peanut allergies from 0.4% in 1997 to 2.0% in 2010. Since 2017, as guidelines spread, rates have started to drop. By 2023, peanut allergy prevalence fell to 1.6% in children, meaning about 300,000 fewer kids are affected than if we’d kept doing nothing.Oral Immunotherapy: Treatment, Not Prevention
Don’t confuse early introduction with oral immunotherapy (OIT). They’re completely different. Early introduction is for babies who don’t have a peanut allergy yet. It’s prevention. OIT is for kids who already have a diagnosed peanut allergy. It involves giving tiny, carefully increasing doses of peanut under medical supervision to build tolerance. It’s not a cure. It’s a way to reduce the risk of a severe reaction if they accidentally eat peanut. OIT can cause side effects like stomach pain, vomiting, or even anaphylaxis during treatment. It’s not something parents should try at home. The American College of Allergy, Asthma, and Immunology (ACAAI) is clear: OIT is not a substitute for early introduction. It’s a treatment for those who already have the allergy. Prevention is still the best strategy.Barriers to Adoption-Why So Few Parents Follow the Guidelines
Despite strong evidence, most high-risk babies still aren’t getting peanut early. A 2022 study in Pediatrics found only 38.7% of high-risk infants were introduced to peanut by age 12 months. Why?- Parental fear: 62% of parents in one survey said they were too scared to try.
- Confusion: Many don’t know how much peanut protein to give or what form to use.
- Doctor gaps: A 2023 survey found only 54% of pediatricians correctly recalled the current guidelines.
- Disparities: Black and Hispanic infants are 22% less likely to get early peanut exposure than White infants, contributing to ongoing allergy rate gaps.

What About Other Allergens?
Peanut isn’t the only food that can trigger allergies. Egg, milk, soy, and tree nuts are common too. The EAT study showed that introducing multiple allergens early-peanut, egg, milk, fish, sesame, and wheat-also reduced the risk of multiple food allergies. It’s not just about peanut. It’s about building tolerance early across the board. But peanut remains the strongest case. It’s the most common cause of fatal food reactions. And the data for early introduction is the most consistent. Other strategies-like taking probiotics or vitamin D during pregnancy-have been studied and shown no real benefit. The only proven method? Feeding peanut early.What’s Next? The Future of Prevention
Researchers are already looking ahead. The PRESTO trial, funded by NIAID and running until 2026, is testing whether even earlier exposure-starting at 3 months-works better for the highest-risk babies. Another study is exploring whether heated peanut powder (which changes the protein structure) might be even safer and more effective. Long-term follow-up from the LEAP study shows the protection lasts. Kids who ate peanut early and then stopped for a year still didn’t develop allergies. That suggests real immune tolerance-not just temporary desensitization. Industry is catching up too. Peanut baby foods have grown 27% a year since 2018. More products are designed specifically for safe, early introduction. And with the FDA now requiring clearer allergen labeling, parents have better tools to make smart choices.Bottom Line: Don’t Wait. Start Early.
If your baby has severe eczema or egg allergy, talk to your doctor by 4 months. Get tested if needed. Then start giving peanut protein three times a week. If your baby has mild eczema, start at 6 months. No test needed. If your baby has no risk factors, just introduce peanut like any other solid food-around 6 months. Don’t use crunchy peanut butter. Don’t give whole peanuts. Don’t wait until they’re two. The window for prevention is narrow-and it’s open right now.The data doesn’t lie. Early introduction works. It’s safe. It’s simple. And it’s saving lives.





12 Comments
Early peanut introduction isn't just smart-it's a public health win. The LEAP study data is irrefutable. Delaying exposure didn't protect kids; it created a generation of vulnerable patients. We've known this since 2017, yet implementation remains inconsistent. Pediatricians need to be proactive, not reactive. Give parents clear, written instructions at the 4-month visit. No jargon. No ambiguity. Just: 'Two teaspoons of smooth peanut butter, three times a week, mixed with water.' Simple. Actionable. Life-changing.
And for high-risk infants, clinic-supervised first exposure isn't overcautious-it's standard of care. Stop treating this like a gamble. It's medicine.
Also, stop using crunchy peanut butter on babies. It's not just unsafe-it's negligent.
Stop waiting. Start feeding.
Okay but like… why are we still acting like this is new? 🤦♂️ I remember my cousin’s kid got Bamba at 5 months in 2016 and now he eats peanut butter straight from the jar. No allergies. No drama. Meanwhile, my aunt still hides peanut butter like it’s contraband and her kid’s 8 now. 😅
Also who decided ‘smooth’ peanut butter was the gold standard? What about peanut flour? Or roasted peanut powder? We’re overcomplicating this. Just give them peanut. Not whole nuts. Not crunchy. But peanut. 🤷♂️
This is beautiful. In Nigeria, we’ve always introduced peanuts early-groundnut soup for babies as soon as they start solids. No one thought twice about it. We didn’t need a 2015 study to tell us what our grandmothers knew. The science just caught up. It’s sad that fear and bureaucracy delayed something so natural. Maybe now, with global awareness, we can stop treating food allergy prevention like a Western invention. It’s a human practice.
And yes, Bamba is the real MVP. Cheap, safe, effective. Everyone should try it.
There’s a deeper truth here that nobody talks about: we’ve been raising kids in fear, not in trust. We shield them from everything-peanuts, gluten, dairy, sunlight-and then wonder why their immune systems don’t know how to function.
This isn’t just about peanut allergies. It’s about how we’ve inverted parenting: safety became the absence of risk, not the presence of resilience.
Early exposure works because it teaches the body to coexist, not to panic. That’s not medicine. That’s biology. And it’s beautiful.
Also, if your pediatrician hasn’t mentioned this by 4 months, ask them why. And if they can’t explain it clearly, find someone who can.
I’m so glad this is finally getting attention! My daughter had eczema and we were terrified to introduce peanuts. But once we did-smooth PB mixed into her oatmeal-and she had no reaction, I cried. Like, actual tears. It felt like we’d passed a test we didn’t even know we were taking. Now she’s 3 and eats peanut butter sandwiches like a champ. Thank you for sharing this. Let’s keep spreading the word. 🙏💛
bro i just gave my son peanut butter at 6 months and he sneezed once and i panicked for 3 days lmao
turns out he was just allergic to dust in the kitchen
you guys are overthinking this. just give em a little smear on the lip and see what happens. if they don’t turn into a balloon, you’re good. 🤙
The immunological mechanism is rooted in epidermal and mucosal dendritic cell priming during the critical window of immune tolerance induction. Early antigen exposure via the gastrointestinal tract promotes Treg differentiation and suppresses Th2 polarization, thereby preventing IgE-mediated sensitization.
What’s fascinating is that the dose-response curve isn’t linear-it’s threshold-dependent. 2g/week is the minimum effective dose; lower amounts show diminished protection. This is why ‘occasional exposure’ fails.
Also, the 2023 meta-analysis confirmed that timing matters more than formulation. Exposure before 6 months yields 98% reduction; after 12 months, efficacy drops to 37%.
And yes, Bamba’s low moisture content and roasted peanut profile may enhance antigen stability. More research needed.
I’m a mom of two. My first kid got peanut at 8 months after a scary visit to the allergist. My second? I started at 4 months, no testing, just smooth PB in yogurt. Zero stress. Zero reactions.
What helped me was realizing: I wasn’t risking my child. I was protecting them. It flipped the whole narrative.
Also-why is it so hard to find peanut powder in the UK? I had to order it online. We need this stuff on shelves. Not just in fancy health stores.
YOU’RE KILLING YOUR KIDS BY WAITING. I SAID IT. I’M NOT SORRY. I’VE SEEN THREE ANAPHYLAXIS CASES IN THE ER. ALL FROM PARENTS WHO ‘WAITED UNTIL THEY WERE OLD ENOUGH.’
THEY WERE 2. ONE WAS AT A BIRTHDAY PARTY. THE OTHER WAS AT A PARK. THE THIRD WAS AT CHURCH.
STOP BEING SCARED. START GIVING PEANUTS.
IF YOU’RE TOO AFRAID, DON’T HAVE KIDS.
While the LEAP study demonstrated statistically significant reduction in peanut allergy incidence, the generalizability to low-risk populations remains unproven. The cohort was highly selected-infants with severe eczema or egg allergy. Extrapolating these findings to the broader pediatric population introduces potential overdiagnosis and unnecessary parental anxiety.
Additionally, long-term adherence data beyond age five is sparse. The clinical significance of the 1.9% vs. 13.7% difference may be overstated in public discourse.
Caution remains warranted in populations without established risk factors.
Wow. So we spent 20 years telling parents to avoid peanuts… and that was the problem?
Like… we’re just now realizing that ‘don’t touch it’ isn’t a strategy?
Reminds me of when we told people not to eat fat and then got an obesity epidemic.
Human beings are terrible at predicting biological outcomes.
Anyway, I gave my kid peanut butter at 5 months. He sneezed. I panicked. He’s fine. I’m still not sure if I did it right.
But at least I didn’t wait until he was 2.
And I didn’t cry in the pediatrician’s office.
So… progress?
The paradigm shift in pediatric allergology reflects a deeper epistemological evolution: from prophylactic isolation to immunological integration. The cessation of peanut avoidance constitutes not merely a clinical adjustment, but a philosophical reckoning with the nature of immunity as a dynamic, not a static, state.
One must ask: if we are to expose infants to allergens, what other biological thresholds are we unlearning? Is the home a sanctuary or a laboratory? Is safety found in absence-or in engagement?
The answer, perhaps, lies not in the peanut, but in the posture of the parent.